Written by Prof Karen Dwyer
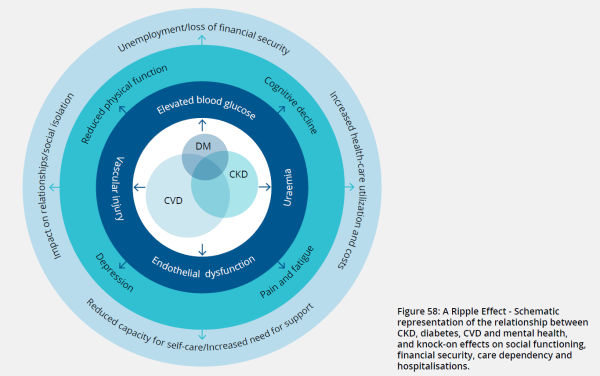
Chronic kidney disease is common, affecting 1 in 10 Australians. The situation is even more dire amongst Indigenous Australians where the prevalence is 1 in 5. Despite this high prevalence, less than 10% are aware they have CKD. This, combined with a lack of symptomatology, means a proactive approach by health care professionals is required. Kidney disease, heart disease including heart failure, and diabetes are common conditions that affect ~30% of the community and frequently occur together. Kidney Health Australia released an evidence report in 2021 (CKD, Diabetes, and CVD: make the link) highlighting the interconnectedness of these conditions. Indeed, diabetes is the most common cause of kidney failure, and the presence of metabolic syndrome is present early in CKD without overt diabetes. Similarly with heart disease, the relationship is bidirectional. Cardiovascular disease increases the likelihood of CKD, and the presence of CKD is a potent risk for cardiovascular disease and death. Kidney disease, cardiovascular disease, and diabetes share aetiologies and pathogenetic mechanisms and the downstream effects also share commonality. The “ripple effect” is nicely shown in the figure below. In short, the most vulnerable are at greatest risk and these conditions further exacerbate disadvantage.
What does this mean for clinical practice?
When someone presents with one of these conditions it is important to think of, and screen for, the presence of the others. Test early for kidney disease if the presenting conditions are diabetes or heart related and consider kidney function in the management of these conditions (particularly around drug dosing). Similarly, when presenting with kidney disease, assess metabolic function and for the presence of cardiac disease and failure.
The interconnectedness of these conditions has been brought to the fore with the release of SGLT2i. These agents confer organ protection particularly with regards to the kidney and the heart even in the absence of diabetes. When started early, these agents can slow the progression of kidney disease and delay reaching kidney failure by years. The economic and personal benefits cannot be underestimated.
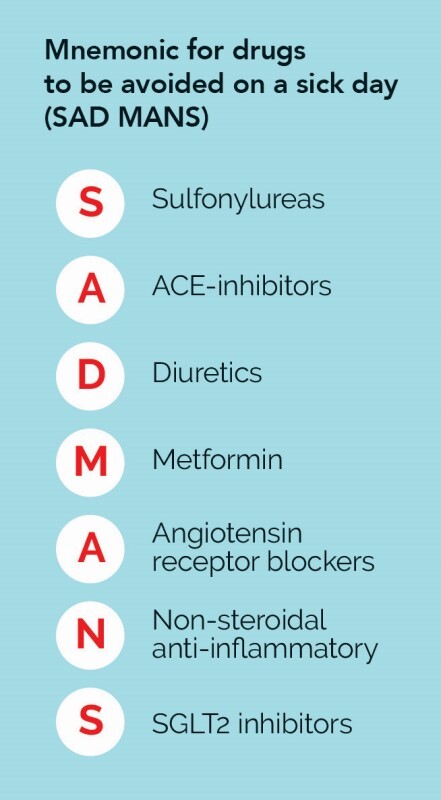
On the 1st September, Dapaglaflozin was granted PBS listing in chronic kidney disease with albuminuria. Added to positive lifestyle behaviour changes and RAAS blockade, such renoprotective therapies can alter the trajectory of kidney disease. Dapaglaflozin may be prescribed for those with CKD on RAAS blockade (streamline authority 13230) with eGFR 25-75ml/min and uACR 22.6 – 565mg/mmol. It is anticipated and expected that there will be a decline in eGFR upon commencement (maximum at 4 weeks) which then rebounds. Upon initiation, I tend to reduce diuretic and potentially antihypertensives depending on the amount of oedema present and blood pressure. Recipients of this drug must be counselled to stop the drug if they experience dysuria; I am cautious in prescribing if there is a history of UTIs. A sick day action plan is critical - the mnemonic SADMANS is helpful in remembering which drugs to stop.
Further discussion on the interconnectivity of kidney disease, heart disease, and diabetes can be found on a podcast series called OrgansTalk released by Boehringer Ingelheim.
Updates to SGLT2i and chronic kidney disease can be found here.

Prof Dwyer is the Clinical Director at Kidney Health Australia and Professor of Medicine and Deputy Head, School of Medicine at Deakin University. She trained as a nephrologist and transplant physician at St. Vincent’s Hospital Melbourne. Prof Dwyer has 15 years clinical experience in the diagnosis and management of renal-related disease, including acute and chronic kidney injury, refractory hypertension and renal transplantation. Prof Dwyer also has an interest in clinical research project specifically surrounding the diabetes arising post transplantation.